The pandemic changed everything. The United States’ first confirmed case of COVID-19 occurred in January, and the virus has rapidly infected 6.5 million people and killed more than 193,000 as of September 15, 2020. A slow federal response increased viral spread, often through asymptomatic carriers, which has harmed people across all walks of life in addition to disproportionately harming our most vulnerable community members. Socioeconomic status often underlines vulnerability to poor health. Cumulative disadvantage, resulting from histories of oppression and domination create conditions for people to act against their own interest. Given these interactions, public health interventions should address the virus itself, and pay special attention to underlying economic inequity, as well as systems of domination which lay upstream from many societal ills.
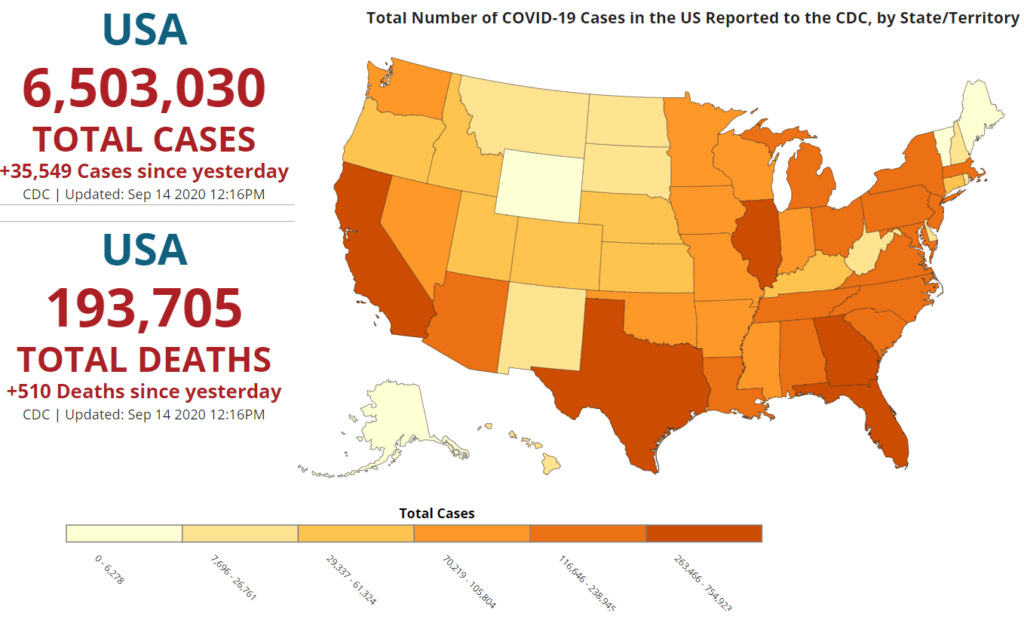
Data Sources, References & Notes: Total cases are based on aggregate counts of COVID-19 cases reported by state and territorial jurisdictions to the Centers for Disease Control and Prevention (CDC) since January 21, 2020, with the exception of persons repatriated to the United States from Wuhan, China, and Japan. The numbers are confirmed and probable COVID-19 cases as reported by U.S. states, U.S. territories, New York City, and the District of Columbia from the previous day.
Key Take-Aways:
- Current inequities in socioeconomic status stem from historical injustices; such disadvantages compound over a lifespan and through generations to cause differential health outcomes, including COVID-19 case and fatality rates.
- Domination, the shaping of another person’s values, beliefs, and desires so they think and act against their interests, creates worsening health conditions among vulnerable populations.
- Public health practitioners must address domination and liberation in interventions related to socioeconomic status and health.
Cumulative Disadvantage and Health
Socioeconomic status can influence what healthcare someone receives, what environments they are exposed to, their health behavior, and levels of chronic stress. In addition, education, income, and occupation all influence health outcomes: education influences what occupation someone enters and, to some degree, their income. In turn, income can be used to purchase health care and to access healthier food, housing, and less stressful environments. In these ways, there is a persistent relationship between socioeconomic status and health outcomes; it follows that initiatives addressing socioeconomic status will make the entire population healthier.
While some may implicitly or explicitly believe economic advantages are a result of work ethic, it is important to recognize that everyone starts out in a different socioeconomic position. Economic disadvantages then compound over time, leading to intergenerational disadvantage which ties the current moment to inequities of the past. For instance, racism and white supremacy created conditions through enslavement, segregation, mass incarceration, and police violence which compound inequity. Gender and sexual minorities face homophobia and transphobia through conversion therapies, stigma, and discrimination, all of which can increase the difficulty of accessing resources through life. In the United States, wealth inequality, driven by income inequality, has increased over the past 50 years((Urban Institute, 2015. “Nine Charts about Wealth Inequality in America,” https://apps.urban.org/features/wealth-inequality-charts/)), with racial disparities continuing to persist (Figure 2). Most strikingly, three individuals own more wealth than the entire bottom 50% (Figure 3). These wealth-based disparities determine who is able to access resources. Cumulative disadvantage creates cycles where a hard life becomes harder, reducing well-being and health across the lifespan.
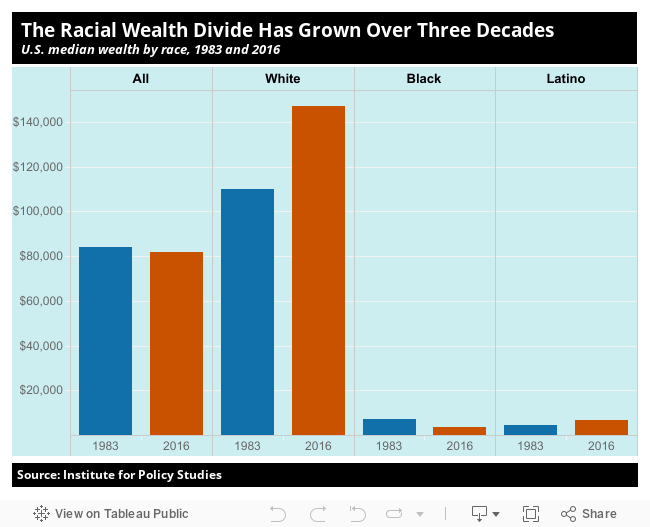
Figure 2 “Racial Wealth Divide,” Inequality.org. Creative Commons License.
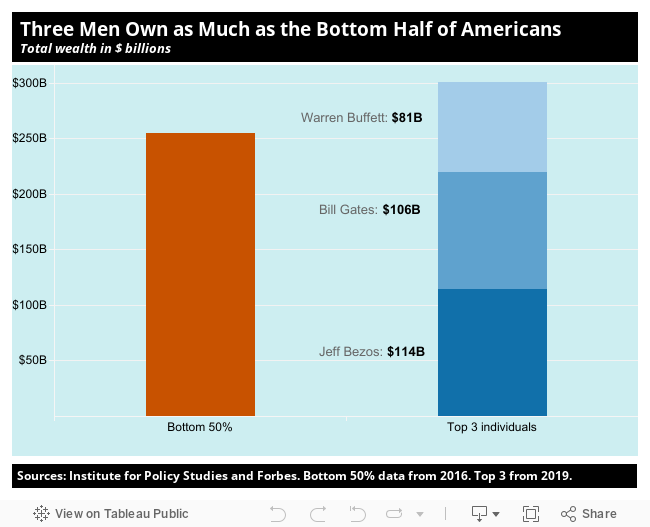
Figure 3 “Wealth Inequality in the United States,” Inequality.org. Creative Commons License.
Socioeconomic Status in the Time of COVID-19
We continue to see how socioeconomic status influences health through the pandemic. Specific populations are more vulnerable to infection, harm, and death from COVID-19 than others. For example, the Primary Care Development Corporation found that COVID-19 case rates were highest in low-income and minority communities in NYC.((Allard, A., Ford, M.M., Manko, K., Weisbeck, K., Cohen, L. (2020). The intersection of COVID-19 and chronic disease in New York City: underscores the immediate need to strengthen primary care systems to avoid deepening health disparities. Points on Care. Primary Care Development Corporation.)) The intersection of COVID-19 and socioeconomic status in New York City underscores the immediate need to strengthen primary care systems to avoid deepening health disparities. In addition, front-line work exposes people to increased risk of infection and ill-health. It has been shown that front-line workers make lower wages on average and come from communities with reduced access to resources, such as primary care, compared to the overall workforce.((Francine D. Blau, Josefine Koebe and Pamela A. Meyerhofer (2020), “Essential and Frontline Workers in the COVID-19 Crisis”,” https://econofact.org/essential-and-frontline-workers-in-the-covid-19-crisis)) The unstable economic environment caused by pandemic-related job loss and business closures, alongside precarious working conditions and accumulated disadvantage, exposes people to increased risk of infection, disease, and death if no safety net exists to support workers.
Legislating Institutional Inequity
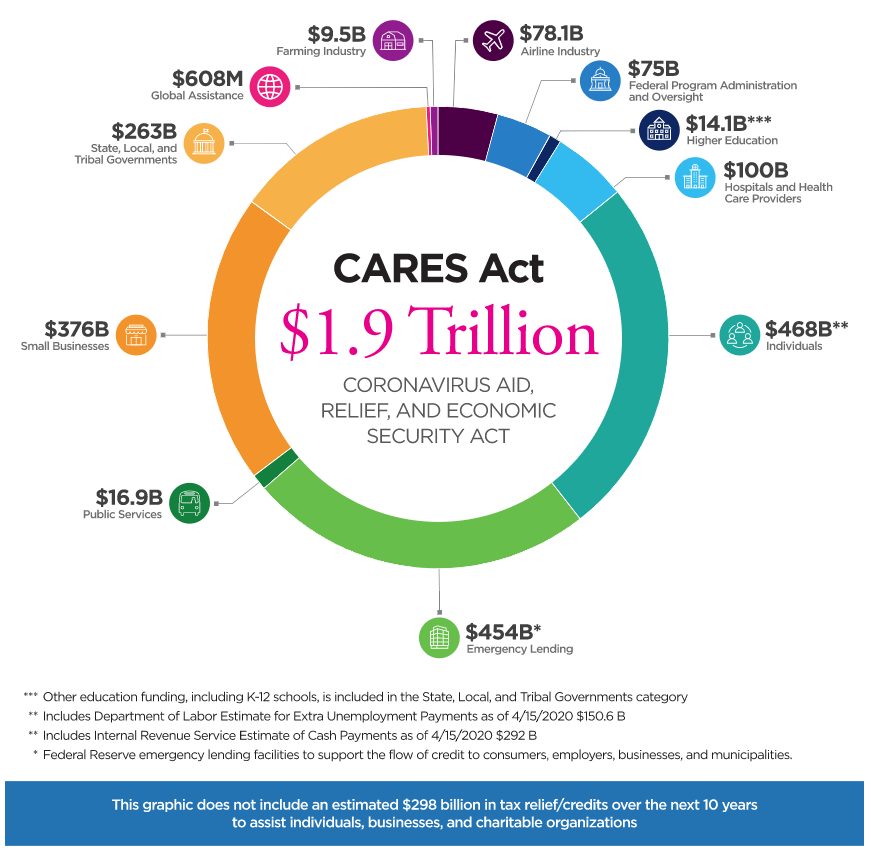
Governmental intervention could reduce these disparities. However, the private sector and governmental institutions in the United States distribute wealth in a highly inequitable way and do not necessarily redistribute accumulated capital and resources to those in need. Oxfam found that 17 of the top 25 most profitable companies, such as Microsoft, Johnson & Johnson, Visa, and Pfizer, are expected to make $85 billion more in 2020 than previous years, with 9 out of every 10 dollars of excess pandemic profits ending up in the hands of white Americans.((Oxfam. (2020). “Who profits from COVID-19, and how can we use that money to help us get a vaccine?” https://www.oxfamamerica.org/explore/stories/who-profits-covid-19-and-how-can-we-use-money-help-us-get-vaccine/)) Technology companies, such as Uber, Google, and Amazon, utilized the pandemic as an opportunity for lobbying for long-held goals, with pharmaceutical companies operating in a similar way.((David McCabe. (2020). How Tech’s Lobbyists Are Using the Pandemic to Make Gains https://www.nytimes.com/2020/04/03/technology/virus-tech-lobbyists-gains.html))((Oxfam. (2020). “Pandemic profiteers exposed” https://www.oxfam.org/en/press-releases/pandemic-profiteers-exposed-report)) On average, the wealth of American billionaires has grown by nearly 25% since the pandemic lockdown started, with average weekly gains of $42 billion which often exceeds the budget deficits of the states they live in.1 The inequity becomes even more striking when analyzing legislative responses. The CARES Act allocated $804 billion for businesses while allocating only $560 billion to household payments and unemployment insurance (Figure 4). In our most dire circumstances, the public institutions that we entrust to protect us allocated more resources towards businesses instead of working people.
Power: Acting Against Our Own Best Interests
Understanding pandemic profiteering at the expense of lives requires an understanding of power and domination. How can we explain how the federal government prioritizes corporate givebacks over people’s health? Why do people end up supporting institutions which go against their best interest? The concept of power gives us a clue. Social theorist Steven Lukes understood power across three dimensions.((Lukes, Steven. Power: A Radical View. London: Macmillan, 1974.)) The first dimension involves someone prevailing in deciding or making decisions that affect another’s well-being. For example, the manager of a restaurant threatening to fire a waiter if he takes a sick day causes the waiter to go to work against his own best interest. Power is also the ability to set the agenda which others follow to make decisions. The owner of a company asks employees to choose between the two cheapest health insurance policies, and the owner blocks any discussion about improving the quality of the coverage. The final, and perhaps most insidious form of power is domination. Domination occurs when people willingly act against their own best interests without any apparent coercion. A working-class person may vote against increasing social welfare programs through taxation because they maintain a philosophical stance on limited government intervention in markets.
Domination is an especially important component for public health professionals to understand. Domination shapes a person’s values, beliefs, and desires in ways that cause them to think and act against their own interests. If we are attempting to identify domination, then we must know what a person’s real interests are. In public health, people in positions of authority can often restrict the freedom and responsibilities of others in the name of someone’s best interests. If a person wants to smoke cigarettes for a nicotine buzz, is it in their best interest to ban cigarettes from preventing lung damage? A cigarette smoker may be a hedonist who values their current sense of pleasure over future pain, which means their smoking may be in their best interest. Identifying and intervening upon domination occurs through our own normative, subjective frames which simply may be different than the frames of others.
What a dizzying cycle! Should we then throw away domination as an analytical tool? Perhaps there is a way out. Allowing people to express a broad range of values related to their lived experience may give a firmer footing: we can aim to identify domination and intervene when someone’s capabilities are reduced. The capability approach dictates that freedom to achieve well-being is important and based on real opportunities to do and be what they have reason to value. The capability to flourish – to experience positive psychological and social functioning – may be another useful tool. We can remove barriers that prevent people from flourishing, such as intervening to reduce racist attitudes that cause discrimination. Lastly, income and wealth can be important empirical measures related to someone’s ability to achieve well-being. While identifying domination so that we can intervene may not be free from postmodern critiques, it can still be a useful tool for public health practitioners.
Power and Domination During COVID-19
It’s important to acknowledge that public health professionals also deploy power in interventions. Public health professionals, backed by empiricism and the scientific method, encourage new ways of interacting to prevent the spread of COVID-19. Nearly everyone in the United States has, at this point, heard of social distancing or utilizing face masks to prevent transmission. A key element to these approaches is that they often rely on changing the day-to-day behaviors of individuals and groups. By encouraging people to wear masks, public health professionals are utilizing their society-granted expertise to create new norms of being in public spaces.
While this aspect of power may have a net positive end (i.e., reducing disease transmission), we must be cautious about how calls for health may be co-opted to increase cumulative disadvantage or cause unintended consequences. Take the two previous examples: pharmaceutical and technology corporations profiteering from the pandemic and frontline workers being exposed to more risk. Or, for instance, policing mask-wearing behavior or fines for people who aren’t wearing a mask may unintentionally cause more disadvantage by increasing the risk of policy brutality or decreasing disposable income required for living among those who live in poverty. Where there is a socioeconomic influence on health, a public health practitioner should evaluate how power and domination may be present. If public health is relying on police, for instance, to enforce a mask mandate, then how do power and domination play a role? Given racial inequalities in policing, does this intervention alleviate or entrench disadvantage?
Another example: public health professionals who aim to seek a return to normalcy. People who agree to wear masks and distance can return to work. The machinery of inequality, however, remains intact. Without changing who owns the means of production, a return to work implies increased income and wealth disparities. In this instance, interventions to reduce disease transmission may simultaneously require interventions providing legal assistance for workers to advocate for personal protective equipment, improving attitudes and beliefs concerning social welfare systems, and applying a wealth tax on pandemic profiteers. Addressing COVID-19 requires addressing socioeconomic status, and addressing socioeconomic status requires addressing power.
Liberation from Domination
Can public health practitioners create interventions that address power inequities and domination? Education is a tool with a strong relationship with domination. When education is controlled and deployed on behalf of capitalist accumulators, it can influence individuals to act against their own best interests. This creates more oppressors alongside more oppressed people. The converse of domination is liberation. Education can support liberation and thus address domination by teaching people the tools to name and critically reflect on the world; to understand that education is political in nature. With tools of critical analysis, people can begin to understand their own best interests and advocate for them against forces of domination.
The pandemic has created opportunities for public health professionals to interact with the public. As professionals, we have the opportunity to create interventions that can improve health and increase skills in critical thinking. While the pandemic exposes the most vulnerable to harm, perhaps we, the people, can gain clarity in understanding how the current systems can be changed to address systematic inequity. By understanding domination, we can find ways to liberate ourselves and others. Through liberation, we can develop social institutions ready and able to embrace human flourishing, happiness, and real empowerment to live through our values.
- Series 4– Public Health Solidarity - September 15, 2020
- Inequity, Domination, and Liberation during COVID-19 - September 15, 2020
- Archive – The Palate, Nutrition and Public Health - July 6, 2020
- Americans for Fair Taxes. (2020). BILLIONAIRES’ PANDEMIC WEALTH GAINS BURST THROUGH $700B. https://americansfortaxfairness.org/issue/billionaires-pandemic-wealth-gains-burst-700b/ [↩]


